
TELEMEDICINE ADOPTION AND DIFFUSION: THE CASE OF
THE UNITED ARAB EMIRATES
Nabeel Al-Qirim
College of Information Technology, United Arab Emirates University, P.O Box 17555 - Al Ain
United Arab Emirates
Keywords: Telemedicine, UAE, Cases, National strategy, telemedicine networks, Mayo Clinic, Abu-Dhabi, Al-Ain.
Abstract: This research was initiated to explore telemedicine (TM) adoption and diffusion in healthcare organizations
in the UAE. According to the exploratory findings of this research, the research endeavored to achieve two
main targets. Initially, it was revealed that the telemedicine phenomenon was not that extensive in the UAE
in the sense there was no self initiated TM networks or specialty TM centers as such. According to this
finding the researcher attempted to explore the perceptions of healthcare professional in the UAE about their
attitudes and behavior towards adopting the TM technology in their organizations using a theoretical
construct extended from the technological innovation literature. Secondly, the existing TM initiatives in the
UAE were initiated in cooperation with Mayo Clinic to have complete multimedia TM system for tele-
consultations (second opinion). The effectiveness of this approach is also examined in this research. The
research discusses the research findings in the light of the overall literature highlighting further implications
and suggesting ways where TM could be pushed forward in the UAE. What is yet to be seen in the UAE
context is the initiation of self governed specialty TM systems and networks.
1 INTRODUCTION
Telemedicine (TM) means medicine from a distance
where distant and dispersed patients are brought
closer to their medical providers through the means
of telecommunication technologies (Charles, 2000;
OTA, 1995; Noring, 2000; Perednia & Allen, 1995;
Wayman, 1994). TM can assist in reaching out to
rural patients (Charles, 2000; Harris, Donaldson, &
Campbell, 2001) and to areas where patient volumes
for certain services are limited (Edelstein, 1999). It
can also assist in implementing administrative and
clinical meetings (i.e., journal discussion, case
discussion), in providing different health-awareness
courses to patients (smoke treatment centers), in
delivering training courses to physicians (discussing
research journal), nurses, and other medical staffs
(Perednia & Allen, 1995; Wayman, 1994), and even
to a level where telemedicine could be used to
promote disease prevention, lifestyle management
and well-being (Lemberis & Olsson, 2003).
TM covers a wide spectrum of benefits in
healthcare through the use of TM utilizing the video
conferencing technology in areas such as
consultations, diagnostics, therapeutic, transfer of
patient related records, case management, training,
and meetings. This mounting hype amongst
researchers and practitioners about TM advantages
lead to a conclusion that TM could be an essential
building block in the strategic plan of many
healthcare organizations (Charles, 2000). In a rural
setting, TM could help health providers in supplying
quality, fast, and economical medical services to
patients including rural ones and hence, saves
doctors and patients valuable time wasted in
commuting large distances (Oakley et al., 2000).
Specialists could utilize this extra time in seeing
more patients at the main hospital.
1.1 Telemedicine in the UAE
Medical services in the UAE has improved
dramatically during the past 30 years where the
number of hospitals increased from 7 to 30, the
number of beds increased from 700 to 4473 and the
number of primary health care centers increased
from 12 to 115 (MOH1)
In the UAE, the term telehealth and TM is not
widely recognized as such. In scanning for
telemedicine initiatives within the UAE, to the best
191
Al-Qirim N. (2006).
TELEMEDICINE ADOPTION AND DIFFUSION: THE CASE OF THE UNITED ARAB EMIRATES.
In Proceedings of the International Conference on e-Business, pages 191-199
DOI: 10.5220/0001426001910199
Copyright
c
SciTePress

of the author’s knowledge, the following
organizations were the only ones reported to adopt
telemedicine projects and applications:
i. Tawam hospital.
ii. Mafraq Hospital.
iii. UAE University (UAEU):
iv. Higher Colleges of Technology (HCT).
The first two are hospitals in the Emirate of Abu
Dhabi and the last two represents an educational
institution. The UAEU has a Faculty of Medicine
and Health Sciences (FMHS) in Al-Ain city and the
HCT provides health-related courses and degree
nationwide.
Given the above stocktaking of the above TM
initiatives in the UAE, it is important to investigate
the potential importance of the TM technology in the
above cases. Therefore, this research attempted to
achieve the following objectives:
i. what are the adopted TM technologies in
these institutions.
ii. where they are being used.
iii. reasons for adoption
iv. challenges facing TM adoption and usage.
v. Extent of adoption and usage of TM.
In the following the research will introduce the
theoretical framework followed by the research
methodology. This is followed by a description of
the cases and the adopted TM technologies. The next
section will show analysis across the different cases
followed by a discussion and a conclusion.
2 THEORETICAL FRAMEWORK
In search for a guiding theoretical framework that
could assist this research in explaining factors
influencing TM success, the classical innovation
diffusion theory (Rogers (1983; 1995) model)
appeared to be the most widely accepted framework
by researchers in identifying critical characteristics
for technological innovations (Moore & Benbasat,
1996; Premkumar & Roberts, 1999; Thong, 1999).
Rogers’ (1995) framework comprised the following
factors: relative advantage, complexity,
compatibility, observability, and trialability. Relative
advantage is the degree to which using technology is
perceived as being better than using its precursor of
practices. Complexity is the degree to which
technology is perceived as being easy to use.
Compatibility is the degree to which using
technology is perceived as being consistent with the
existing values, and past experiences of the potential
adopter. Trialability is the degree to which
technology may be experimented with on a limited
basis before adoption. Observability is the degree to
which the results of using technology are observable
to others. Rogers’ (1995) compatibility characteristic
is highly envisaged here as past studies (Austin,
1992; Austin, Trimm, & Sobczak, 1995) have
considered the problem relating to physicians
accepting information technology (IT) for clinical
purposes. Cost was outlined as an important factor
by other researchers (Bacon, 1992; Elliot, 1996;
Tornatzky & Klein, 1982). Cost means the degree to
which technology is perceived as cost effective. The
image factor was found important to the adoption of
technologies in the health literature (Little &
Carland, 1991). Image means enhancing one’s
image or status in one's social system. Even-though
Rogers (1995) highlighted the importance of the
image factor on IT adoption he suggested that it
could be studied from within the relative advantage
characteristic. However, Moore and Benbasat (1996)
stressed the image factor as an independent factor on
its own. As TM projects involve considerable
investments, top management support is viewed as
important to the adoption decision (Kwon & Zmud,
1987).
2.1 Determinants of TM Adoption
In review of more recent literature it was observed
that despite the rapid growth and high visibility of
TM projects in health care (Grigsby & Allen, 1997),
few patients were actually being seen through the
TM for medical purposes. In almost every TM
project, tele-consultation accounts for less than 25%
of the use of the system (Perednia & Allen, 1995).
Other research reported mid-level success for
telemedicine projects (Guedemann, 2003). In a large
study in the US, Edwards and Patel (2003) found
that the clinical uses of the telemedicine network did
not exceed 30%. The majority of the online time was
used for medical education and administration
(Edwards & Patel, 2003; Wayman, 1994; Perednia
& Allen, 1995; Hassol, 1996). Earlier success stories
of telemedicine in countries such as the US
demonstrated that telemedicine was feasible while
maintaining diagnostic accuracy, which challenged
the widely held belief that a patient and a provider
must be in close proximity for healthcare to take
place.
The important unresolved issues revolve around
how successful TM can be in providing quality
healthcare at an affordable cost and whether it is
possible to develop sustainable business model that
would maintain profitability over time. This depends
on (Perednia & Allen, 1995): (1) clinical
ICE-B 2006 - INTERNATIONAL CONFERENCE ON E-BUSINESS
192
expectations, (2) matching technology to medical
needs, (3) economic factors like reimbursement, (4)
legal (e.g., restrictions of medical practices across
state lines (licensure) and issues of liabilities), and
social (e.g., changing physician behaviors and
traditional practices and workflow) issues
(Anderson, 1997), and (5) organizational factors.
Edwards and Patel (2003) attributed the success of
TM projects to defined clinical needs, organizational
support, physicians’ and patients’ acceptance,
exhibiting measurable cost and clinical benefits, and
moving toward sustainable operations. Interestingly,
Whitten et al. (2002) in a comprehensive study
concluded that there is no evidence that TM is a cost
effective mean of delivering healthcare.
In their review of the literature, Finch et al.
(2003) supported the above factors and found the
following hurdles which could increase the
resistance to telehealthcare in practice:
i. telehealthcare is somewhat unstable.
ii. there are some concerns relating to the
doctor-patient interaction.
iii. concerns about clinical risk and potential
litigation
iv. at an international level, some difficulties
relating to licensure and reimbursement were
reported.
v. the production of evidence about the safety
and effectiveness of telehealthcare
vi. despite the numerous trials of telehealthcare
in Britain and elsewhere, such services
typically fail to become part of routine
healthcare delivery.
3 METHODOLOGY
This research is exploratory in nature in the sense
that there is no prior research in UAE to guide this
research in achieving the above objectives. Case
studies are appropriate for the exploratory phase of
an investigation (Yin, 1994). Therefore, this research
will follow the qualitative paradigm by adopting
Yin’s (1994) hard case-study methodology.
Yin’s (1994) positivist approach is acceptable by
the interpretivist school as well. For example,
Walsham (1995) indicated that although Yin (1994)
adopted an implicit positivist stance in describing
case study research, his view that case studies are
the preferred research strategy to answer the above
type of questions would also be acceptable by the
interpretive school. Details of the different cases are
provided in the following section.
Interviews were sought from many experts
involved in telemedicine projects in the UAE. Those
experts were: educational, specialists/surgeons, IT
and administrators/managers (Table 1). Those
experts were requested (after explaining the research
objectives and content) to complete a qualitative
survey questionnaire. Site visits were implemented
to FHMS and Tawam to see TM installations and
meet respondents.
Table 1: Respondents’ distribution across the different
cases.
Case Number
of respondents
UAE University 3
Tawam Hospital 4
Mafraq Hospital 1
4 THE CASES
4.1 FMHS
FMHS in UAEU uses the video conferencing
technology to deliver classes to male and female
students separately as classes are unisex and mixed
classes are not allowed within UAEU. Faculty
member alternate between female and male classes,
usually synchronized to take place at the same time.
For example, if a faculty member existed in the male
class; female students attend the same session in an
adjacent classroom through the video conferencing
link across the two classes.
4.2 Tawam Hospital
Tawam Hospital2 TM project represents a
partnership between UAE Ministry of Health and
Mayo Clinic (Rochester, Minnesota, USA).
Implementation started in September 2000 and first
case was sent in February 2001. The developers are
Mayo Clinics IT and Mayo Office of Middle East
Healthcare and Mayo subcontractor – Wellogic,
Boston, USA. Tawam TM technologies include: 512
Internet leased line; direct text captures entry;
digitized transparent images i.e X-rays, CT, MRI,
nuclear med, ultrasound, clear prints; digitized
reflective images, i.e. any paper print, document,
item needing scanning; CD drive to attach directly
still and motion films in DICOM format;
video/Audio conferencing; and fax.
The TM system is designed to handle
complicated patient consultations with the ability to
TELEMEDICINE ADOPTION AND DIFFUSION: THE CASE OF THE UNITED ARAB EMIRATES
193
transmit multimedia clinical information. Item that
can be transmitted include: Scanned paper medical
records; scanned X-ray films; digitized
echocardiography video; digitized cine-angiography;
and live videoconferencing.
There are four user groups that work closely
together to accomplish a TM consultation. These
groups include: UAE site requesting, UAE
telemedicine office coordinator; Mayo clinic
telemedicine office coordinator; Mayo clinic
consulting physician. Tawam adopted a standard
with Mayo clinic concerning reporting and receiving
patient consultations. Tawam reported that on
average, 4 cases were reviewed each month with
Mayo clinic.
Recently, Tawam established a large scale video
conferencing centre with the capability to have
simultaneous video sessions with several online
locations for meeting and educational purposes. The
centre will serve many clinical and administrative
staff as Tawam has signed with several international
medical centers and institutions to provide training
courses.
4.3 Al Mafraq Hospital
Similar to Tawam’s TM system where on November
1996, The Ministry of Health signed an agreement
with Mayo Clinic Foundation, Rochester,
Minnesota, USA to receive technical advice and
support in the design and construction of a TM
system to link three referral hospitals in Abu Dhabi,
Al Mafraq and Al Ain with Mayo Clinic for medical
e-consultation. As commented by one of the
respondents, “the TM system will be suitable for
store and forward as well as “real time”
communication link” and will be based on Mayo’s
experience of maintaining the integrity of patient
data, static images and full motion studies during the
process of digital acquisition, processing,
transmission and reconstruction. However, Mafraq
Hospital favored the “store and forward” option
more than the videoconferencing one as it does not
require that partners be present at the same time.
This is important specially if there is a time
difference between the two remote sites. Mafraq
implemented the solution using 512k internet link
through its Wide Area Network.
5 CROSS CASE ANALYSIS
Tawam and Mafraq adopted the same TM system
from Mayo clinic and hence, similar views were
unified into one depiction in this research in order
not to repeat reporting the same findings twice.
However, Tawam has adopted another large video
conferencing centre for education and meeting
purposes which could differentiate their responses
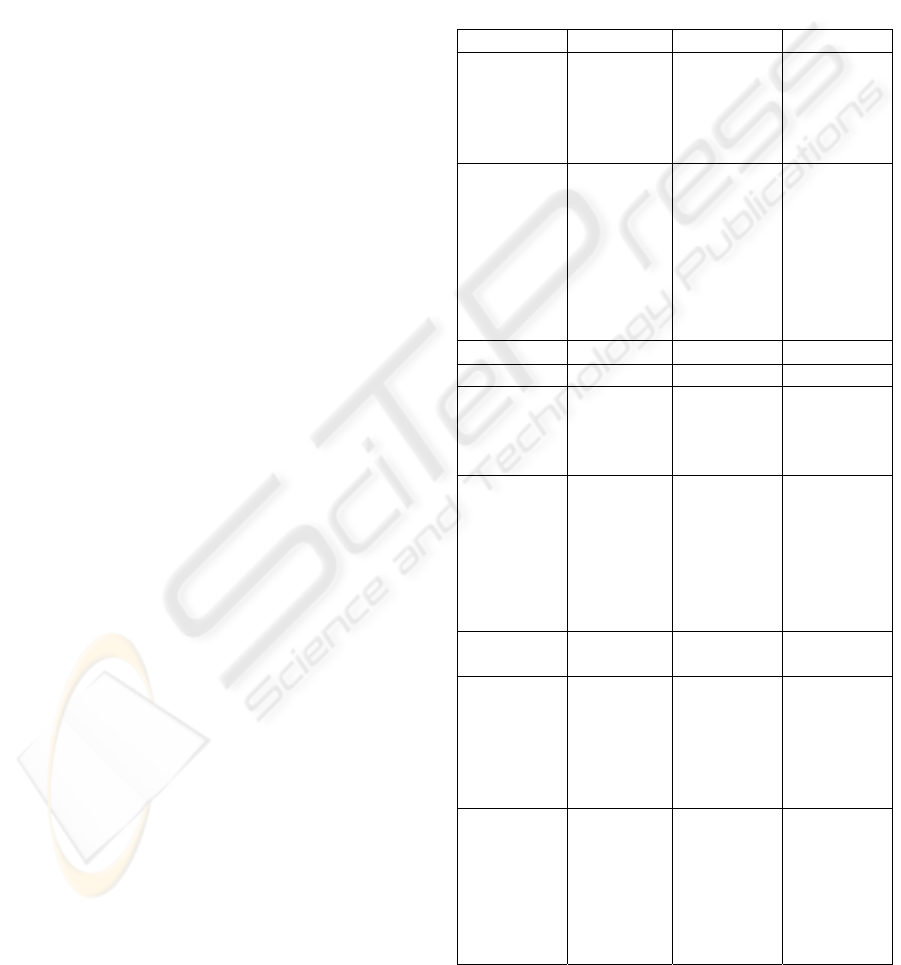
from Mafraq hospital. Table 2 summarizes the
research findings and analysis across the different
cases.
Table 2: Research findings and analysis across the
different cases.
Issue UAEU Tawam Mafraq
Advantages
Education Consultations
with Mayo
clinic
Education
Consultations
with Mayo
clinic
Complexity Not complex
Training and
onsite
support
should
remove any
complexities
Not complex
Not complex
Compatibility Compatible Compatible Compatible
Observability Important Important Important
Trialability Important
but difficult
to
implement
Important Important
Cost Not
important
An issue if
going to
bigger TM
projects
Not
important
Not
important
Image
Moderate
effect
Important Important
Top
Management
Support
Important
Simple
decision
process and
structure
Important -
role of the
Government
Important
UAEU
leading role
to encourage
others to
adopt TM
- -
ICE-B 2006 - INTERNATIONAL CONFERENCE ON E-BUSINESS
194

Most notably, the relative advantages and the
compatibility factors attracted most of the
discussions amongst the different cases. Those are
explained next.
5.1 The Relative Advantages
All cases retained positive view about the potential
and the applications of TM in different departments
in their hospitals. The main issue raised by Tawam
is that some hospitals may not have the capabilities
and the needed resources to diagnose for specific
illnesses where TM could play a vital role here –
where they highlighted the following advantages:
i. Expanding the reach of the medical services
you can provide
ii. Reducing the costs associated with
unproductive travel
iii. Saving time away from clinical or educational
practice
iv. Sharing medical knowledge throughout
dispersed groups
v. Maintaining professional certifications without
going off-site
vi. Increasing team interaction, and improving
work flow and quality
vii. Sharing images easily for quick consultations –
across desktops
However, due to the educational role of FMHS,
they envisioned using the TM system for educational
purposes only, commenting “thus, the main focus of
telemedicine in FMHS is centred more on educating
future physicians than on providing immediate
medical service to patients outside the teaching
hospitals”. The same respondent commented that
“we have the specialists and the technology; we just
don’t have the mandate. We can, however, provide
specialty education in the way of CME to physicians
at a distance. The other specialty service that we
could provide to the Health Authority (and
physicians at a distance) is assessment of basic
competency skills through online exams (similar to
the Canadian Medical Council exam and the US
Medical Licensing Exam).” In addition, another
respondent from FMHS indicated that TM could be
used to supervise junior doctors or nurses in a
remote place, virtual attendance at overseas
conferences, importing/inviting conferences from
overseas, employment interviews and examining
research theses. This respondent confirmed that
these practices using have been implemented since
1994.
By adopting TM the hospitals (cases) could
provide health consultations to areas that these
services are not available. Mafraq hospital indicated
that the TM technology enables an electronic patient
visit virtually to Mayo Clinic without the
inconvenience and cost of traveling overseas. TM
delivers telehealth care services to hospitals like
Mafraq and Tawam Hospitals in the UAE for
medical consultation, referral, and second opinion. It
captures medical information electronically,
compress and transmit high-end resolution images,
digital full motion videos like angioplasty
procedures, colonoscopy, electronic EEG, MRI, CT
Scan, X-ray films, laboratory reports, and Digital
Clinical Still and Video Images.
Another respondent from Tawam confirmed that
TM could make specialty care more accessible to
underserved rural and urban populations in the UAE.
Video consultations from a rural clinic to a specialist
can alleviate prohibitive travel and associated costs
for patients. Videoconferencing also opens up new
possibilities for continuing education or training for
isolated or rural health practitioners, who may not be
able to leave a rural practice to take part in
professional meetings or educational opportunities.
Mafraq supported the same and raised other
advantages as well:
i. Provide more access to patients and families by
reducing the need for travel during severe
weather conditions.
ii. Reduce expense to patients and their families as
well as the UAE government at the hospital
level:
a. reduce travel distance & time away from
work/home for patients/families
b. provide a more efficient use of hospital
staff.
The other cases emphasized that they could
utilize TM in consultations, diagnostics, therapeutic,
in-surgery, transfer of patient related records, case
management, training & meetings (clinical/admin.).
One respondent from Tawam hospital envisioned
TM to be used in all clinics. Another respondent
from Tawam specified that TM could be used in
neurology, dermatology, gen/surgery, gastrology,
haematology, special Service, internal medicine,
ophthalmology, orthopaedic, urology, pediatrics and
gyn.
5.2 Compatibility
As for the compatibility aspect of the TM
technology, the cases did not view TM as
incompatible with them as such. For example, the
case of FMHS did report some issues concerning old
staff accepting the TM technology and
TELEMEDICINE ADOPTION AND DIFFUSION: THE CASE OF THE UNITED ARAB EMIRATES
195

administrative staffs were more comfortable using
the TM technology than doctors. However, such
incompatibilities could be reduced by providing
minimal training in order to build up experience
professional responsibility amongst faculty
members. With time, all clinical and administrative
staff would be encouraged to use TM.
The case of FMHS further commented that
change as a result of introducing new technology is
always difficult for some people. This is particularly
important in the case of people who feel they are
already stretched out with duties and tasks (like most
doctors). The case pointed that change could be
accelerated if there is clear and significant advantage
of using TM to doctors commenting, “they will be
motivated to change.” For example, medical faculty
staff had to learn how to lecture in simultaneous
video classrooms and had no trouble in dealing with
the TM technology. The majority of those faculty
members were quite proficient at using the
technology and adapting their teaching style to the
new environment – although the case of FMHS
admitted that faculty members had no choice but to
use the TM technology in running the simulcast
video classrooms commenting, “so that made the
need for adoption strongly convincing!.” FMHS
noted that more recent graduates were quite
comfortable with technology commenting “I believe
they will be the models for the use of technology in
medicine.”
Tawam strongly believed that by giving the TM
technology the chance to operate inside the hospital,
the staff will get used to it. Although Tawam
admitted that TM should be used more frequently by
doctors and administrators. The same respondent
indicated that TM could fit in easily amongst the
different technologies inside the hospital, i.e.,
integrate with Hospital Information System (HIS).
Other specific incompatibilities were reported as
well. From example, Tawam indicated that the still
video conferencing feature was not active due to
time difference between UAE and the US. Tawam
hospital reported that it was looking into signing
agreements with other known medical centers that
do not have significant time differences with them.
Also, they raised security concerns in sending
patient information over non-secure channels as one
of the impediments.
As for the compatibility of the TM with patients,
the cases pointed that this issue could be one of the
most difficult hurdles to overcome with respect to
the accuracy of diagnosis commenting “when 70%
of diagnoses are made from the patient interview, it
seems critical to be able to elicit this same amount of
information from patients using the TM
technology.” The case perceived that such expected
incompatibility could be reduced if there is a support
person in the room with the patient, such as a nurse,
this might help the patient to become more
comfortable. Tawam confirmed the same by
commenting “if it was necessary to have TM in the
remote location then yes.”
Another interesting issue reported here is that
patients favored traveling overseas over using the
Mayo clinic remote consultation service.
6 DISCUSSION
6.1 The Significance of the Research
Model
It was clear that the decision to adopt TM was
motivated by the relative advantage specifically, its
compatibility, lack of complexity, observability,
trialability, image enhancement to the cases, top
management support and the role of the government
in playing a leading role in the country for other
hospitals to follow. The cases have reported many
advantages as a result of adopting the TM
technology as detailed above. Although cost was
viewed as unimportant to the adoption decision of a
medical tool but it would play a role if the cases
opted to expand their TM initiatives beyond the
current simple TM technology in
collaboration/cooperation with Mayo clinic in the
US.
The different factors in the research model have
helped is shedding interesting light on the adoption
and usage of TM in the different cases. Most of the
factors appeared as positively motivating the
adoption decision of TM (Table 2). The implications
arising from this positivism are twofold. Initially, it
could be argued here that such positive views
represent a good foundation for the large scale
adoption of TM in the UAE and indeed, such simple
and imported “know-how” and successful initiatives
could facilitate the adoption of more complex TM
initiatives at the national level in the UAE.
However, this could only be judged upon initiating
such projects within the UAE first. Secondly, such
positivism was expected given the limited scope of
the adopted TM technology in the hospital-cases.
The lack of more comprehensive and interactive TM
initiatives in the UAE (networks of TM projects,
involved specialist in TM consultations in rural
settings, collaborative/cooperative TM initiatives
ICE-B 2006 - INTERNATIONAL CONFERENCE ON E-BUSINESS
196

across hospitals and universities, etc.) could have
contributed to such response by the case. This
conjuncture could be supported or refuted upon
implementing such advanced TM initiatives in the
UAE. This is yet to be seen.
However, such finding does not undermine the
importance of the depicted framework as it helped in
gauging the respondents concerning different
important issues surrounding the adoption and
diffusion of the TM technology in their
organizations. Thus, it is important to keep
monitoring the progress of TM in the UAE
alongside the research factors and whether any
serious national initiative is being activated in
response to the above suggestions. This raises the
importance of conducting longitudinal research in
order to monitor and report such progress.
6.2 The Compatibility of TM
The compatibility factor attracted a lot of the
discussion in this research and indeed, policymakers
need to introduce training programs to address the
emergence of such possible incompatibilities
between people working in the health sector and
technologies in general and TM technologies more
specifically. Part of the compatibility factor, security
was raised as one of the impediments to the adoption
decision of TM and hence, introducing more secure
measures to protect data and people across the video
link could warrant against any breaches or hacking
activities.
Given the time difference between the UAE and
the US, the Mafraq and Tawam hospitals favored the
“store and forward” option more than the
videoconferencing one. Also it was convenient to
both hospitals as this solution does not require that
partners be present at the same time. However, this
limiting aspect needs to be resolved in order to
maximize the utilization of the TM technology to the
benefit of the hospitals in the UAE. The cases
suggested some solutions where for example,
Tawam hospital reported that it was looking into
signing agreements with other known medical
centers that do not have such significant time
differences with them. However, the suggested
national initiative could address such perspective
more effectively.
6.3 Research Implications and
Suggestions
The research findings lead to a conclusion that TM,
as a medical tool, is being adopted minimally in the
UAE context. Its use for educational and
administrative purposes is well noted across the
different cases. Indeed, this is one of the important
tools of TM but due to its strategic importance in the
healthcare area and to the fact that the UAE have
several rural areas and communities, it was expected
that the potential use of TM in serving these
communities was more extensive.
Accordingly, the implications here are twofold.
Initially, the use of this TM system seemed ideal in
this context (consultation and providing second
opinion). On the other hand, the second implication
points to the importance of exploring the effective
use of the TM in different areas – more specifically:
i. In an internal and rural settings. Healthcare
providers in the UAE need to consider
establishing TM initiatives that could
capitalize on existing medical specialties
and services within the country and devise
ways to integrate TM into these services.
This tight coupling between the TM
technology and medical practices is the
only way for TM to succeed in the UAE.
Providing TM services at the outset or in
parallel to existing medical services will
waive its importance as an efficient
technique or as a replacement to existing
inefficient/old medical practices or
services.
ii. In a regional setting. The potential
advantages of such effective medical and
social TM networks could have a profound
impact on the health and the wellbeing of
people within the UAE. This is of great
importance to the UAE’s context given the
extant geographical dispersion of the
different Emirates in the Federation, cities
and rural areas/towns.
TM could play a vital role in bridging many
gaps:
i. Shortage in specialty staff in rural areas.
ii. Shortage in specialty staff in main centers
(where Mayo clinic link is well justified here).
iii. Moving patient from rural areas to specialists
in main hospitals.
iv. Commuting specialist to rural health centers.
Encouraging linkages
(collaboration/cooperation) with other health centers
within the UAE to share resources, expertise and
knowledge. This could lead to the establishment of
specialty centers in certain health fields.
Running such TM networks could yield
monumental economies of scope/scale in the
medium to long term projections and could prove to
TELEMEDICINE ADOPTION AND DIFFUSION: THE CASE OF THE UNITED ARAB EMIRATES
197

be an efficient and an effective medical tool in the
UAE. The current TM systems in the UAE
represents an initial and a vital resource for such
networks as the quality of consultations provided by
such specialty centers like Mayo clinic represent a
climax in the area of healthcare in the world. At the
regional level, such TM networks could establish the
UAE as a leading healthcare destination. The UAE
is well qualified to occupy this position given the
witnessed economical, technological and educational
growth and the stable political and legal
environment. The culture and the social environment
in the UAE is characterized of being as open to other
cultures. However, learning from the experience of
other medical destinations in the region (i.e., Jordan,
Kuwait) is very important. Hurdles concerning the
TM technology such as obtaining approvals and
certifications of the TM equipment (i.e., from the
FDA), reimbursement, litigations, and licensure are
big concerns in the US but not to the UAE context.
These issues provide further drive to the adoption of
TM in the UAE.
The amount of resources provided by the
government to the adoption of latest techniques and
tools in healthcare are tremendous and indeed, TM
could be considered as one of these strategic
projects. Indeed, this alone could remove many of
the hurdles surrounding justifying the financial
efficacy of the TM in healthcare in the UAE. Such
hurdles at the beginning of any TM projects could
kill the project at its infancy.
What is yet to be seen is to push the current TM
initiatives into the more interactive ones (TM
networks). Of course, providing a strategy for the
effective use of such networks is very important as
well. Looking for leaders and product champions in
each hospital is very important. This fact was also
supported in this research. Given the technical and
social complexity of the TM technology, leaders and
product champions could play a vital role in
empowering and facilitating the adoption and the
usage of TM in their organizations in the UAE.
It could be argued/agreed here that the UAE
government is engaged in executing more urgent
projects (infrastructural) but that should not
undermine the fact that TM could be considered as
one of such priority/strategic tools. This is yet to be
seen as well.
7 CONCLUSION
This research has addressed many of the issues
surrounding the adoption and usage of TM in the
UAE from a theoretical and a professional stance
and pointed to several implications and suggestions.
Such findings are of great importance to
professional, policymakers and researchers
interested in the research findings in general or in
the UAE context more specifically. The research
calls upon such stakeholders to initiate more
comprehensive and interactive TM projects in the
UAE and to consider the TM technology as one of
the strategic building blocks of the national health
strategy in the UAE. Thus, elevating beyond the
current simple use of the TM technology and hence,
emancipating into more daring TM initiatives could
benefit the health sector in the UAE. This may not
necessary take the form of “big-bang” project and
indeed, such national initiative could be achieved in
phases. The research findings set broad guidelines
and suggestions for such stakeholders and indeed
more consequent research studies could monitor the
progress and the development of the TM technology
and the research model in the UAE.
REFERENCES
Anderson, J. (1997). Clearing the Way for Physicians: Use
Of Clinical Information Systems. Communication of
the ACM, 40(8), 83-90
Austin, C. (1992) Information Systems for Health Services
Administration. Michigan: AUPHA Press/Health
Administration Press.
Austin, C., Trimm, J., & Sobczak. P. (1995). Information
Systems and Strategic Management. Healthcare
Management Review, 20(3), 26-33.
Bacon, C. (1992, September) The Use of Decision Criteria
in Selecting Information Systems/ Technology
Investments. MIS Quarterly, 369-386.
Charles, B. (2000). Telemedicine can lower costs and
improve access. Healthcare Financial Management
Association, 54(4), 66-69.
Edelstein, S. (1999). Careful telemedicine planning limits
costly liability exposure; Healthcare Financial
Management, 53(12), 63-69.
Edwards, M.& Patel, R. (2003). Telemedicine in the state
of Maine: A model for growth driven by rural needs.
Telemedicine Journal and eHealth, 9(1), 25-39.
Elliot, S. (1996). Adoption and Implementation of IT: An
Evaluation of the Applicability of Western Strategic
Models to Chinese Firms. In Kautz, K., & Pries-Heje,
J. (Eds.), Diffusion and Adoption of Information
Technology (15-31). London: Chapman & Hall.
Finch, T., May, C., Mair, F., Mort, M. & Gask, L. (2003).
Integrating service development with evaluation in
telehealthcare: An ethnographic study. BMJ (327), 22
November, 1205-1209.
Grigsby, B. & Allen, A. (1997). 4th annual telemedicine
program review. Telemedicine Today, 5(4), pp. 30-42.
ICE-B 2006 - INTERNATIONAL CONFERENCE ON E-BUSINESS
198

Guedemann, M. (2003). Success in telemedicine: Some
empirical evidence. Telemedicine Journal and e-
Health, 9(1), 1-2.
Harris, K., Donaldson, J. & Campbell, J. (2001).
Introducing computer-based telemedicine in three
rural Missouri countries. Journal of End User
Computing, 13(4), 26-35.
Kwon, T., & Zmud, R. (1987). Unifying the fragmented
models of information systems implementation. In
Borland, R. & Hirschheim R. (Eds), Critical issues in
information system research (252-257). New York:
John Wiley.
Moore, G., & Benbasat, I. (1996). Integrating Diffusion of
Innovations and Theory of Reasoned Action Models to
Predict Utilisation of Information Technology by End-
Users. In Kautz, K., & Pries-Heje, J. (Eds.). Diffusion
and Adoption of Information Technology (132-146).
London: Chapman & Hall.
Lemberis, A. & Olsson, S. (2003). Intelligent biomedical
clothing for personal health and disease management:
State of the art and future vision. Telemedicine Journal
and e-Health (The Journal of the American
Telemedicine Association), 9(4), 379-386.
Little, D., & Carland, J. (Winter 1991). Bedside nursing
information system: A competitive advantage.
Business Forum Winter, 44-46
Noring, S. (2000). Telemedicine and Telehealth:
Principles, Policies, Performance, and Pitfalls.
American Journal of Public Health, 90(8), 1322.
Oakley, A., Kerr, P., Duffill, M., Rademaker, M., Fleisch,
P., Bradford, N. & Mills, C. (2000). Patient cost-
benefits of realtime teledermatology – a comparison of
data from Northern Ireland and New Zealand. Journal
of Telemedicine and Telecare, 2, 97-101.
Office of Technology Assessment U.S Congress (OTA)
(1995). Bringing Health Care On Line: The Role of
Information Technologies, OTA-ITC-624.
Washington, D.C: US Government Printing Office.
Perednia, D., & Allen, A. (1995). TMVC Technology and
Clinical Applications. The Journal of the American
Medical Association (JAMA), 273(6), Feb. 8, 483-
488.
Premkumar, G., & Roberts, M. (1999). Adoption of New
Information Technologies in Rural Small Businesses.
The International Journal of Management Science
(OMEGA), 27, 467-484.
Rogers, E. (1983). Diffusion of Innovation.. New York:
The Free Press.
Rogers, E. (1995). Diffusion of Innovation.. New York:
The Free Press.
Thong, J. (1999). An integrated model of information
systems adoption in small business. Journal of
management information systems, 15(4), pp. 187-214.
Tornatzky, L., & Klein, K. (1982). Innovation
Characteristics and Innovation Adoption
implementation: A Meta-Analysis of Findings. IEEE
Transactions on Engineering Management, 29(11), 28-
45.
Walsham, G. (1995) Interpretive case studies in IS
research: Nature and method. European journal of
Information Systems, 4, 74-81.
Wayman, G. (1994). The maturing of TMVC technology
Part I. Health Systems Review, 27(5), 57-62.
Whitten, P., Mair, F., Haycox, A., May, C., Williams, T.
& Hellmich, S. (2002). Systematic review of cost
effectiveness studies of telemedicine interventions,
BMJ (324), 15 June, 1434-1437.
Yin, R. (1994). Case Study Research Design and Methods.
California: Sage Publications.
1
(MOH) Retrieved on 15/12/2005 from the web:
http://www.moh.gov.ae/
2
(TAWAM) Retrieved on 17/12/2005 from the web:
http://www.tawam-hosp.gov.ae/
TELEMEDICINE ADOPTION AND DIFFUSION: THE CASE OF THE UNITED ARAB EMIRATES
199
